Sleep: effective ways to improve it
By Ben Williamson @ 2021-11-15T14:42 (+142)
Introduction
Our research found that melatonin supplementation, cognitive behavioural therapy for insomnia (CBT-I), light regulation, mindfulness-based stress reduction (MBSR), and improved night-time air circulation could all be effective ways for you to increase the quality and quantity of your sleep.
This is a summary of research conducted into the most worthwhile practices for sleeping better. The post is the first in a series looking into the most effective ways people can improve their wellbeing, aiming to present this information as simply and practically as possible.
Thanks to the EA Infrastructure Fund for financing this project. If you find this information useful and/ or take up any of the suggestions, please let me know in the comments or a personal message!
Important note: None of the following constitutes professional medical advice. Some of the interventions suggested have risks of negative side effects that are discussed below. We encourage you to experiment with these practices but please be cautious in doing so and take any risks seriously.
Top takeaway
Our principal recommendations for improving sleep quality are (in order):
- Melatonin supplements: 0.3mg (300mcg) daily taken two hours before bed.
- CBT-I: a six-to-seven-week, self-guided course in cognitive behavioural therapy for insomnia, accessed through an app.
- Light therapy: greatly increasing exposure to bright light during the day, either through building a lumenator or purchasing a SAD lamp.
- Improved night-time air circulation: opening a window to reduce overnight CO2 accumulation.
- Mindfulness-based stress reduction: mindfulness training through an app with a focus on sleep.
Key Findings
Following a broad search of possible interventions, this review evaluated the effectiveness of 11 practices for improving sleep quality and quantity using an adapted weighted factor model.[1]
The five most promising interventions are listed below along with a brief explanation. More detailed assessments of all 11 practices are provided further down.
This research compared interventions across six criteria: strength of evidence, quality of evidence, ease of implementation, risk, externalities, and novelty. Full results from the model, along with reasoning for the metrics used and their respective weightings, can be found here.
Melatonin
Ranking: 1st
Intervention: 0.3mg daily supplementation (e.g. Options A, B and C)
Summary: Melatonin is a natural sleep hormone that can improve sleep quality and quantity when taken in small, daily doses. Melatonin supplementation appears highly practical, with a low risk of notable side effects as well as possible spillover benefits for other conditions.
CBT-I
Ranking: 2nd
Intervention: Completion of an app-based CBT-I course (e.g. Dozy; CBT-I Coach)
Summary: Cognitive Behavioural Therapy for Insomnia (CBT-I) involves a combination of reframing negative thoughts around sleep, improving sleep hygiene, and implementing sleep restriction. We found good evidence that completing a self-guided CBT-I course via an app can be an effective way to sleep better.
Light therapy
Ranking: 3rd
Intervention: Increasing indoor lighting brightness, preferably up to 10,000 lux or more (e.g. a ‘lumenator’ or a Seasonal Affective Disorder [SAD] lamp).
Summary: Multiple studies have found that significantly increased exposure to bright morning light improves sleep quality and quantity. We found negligible risks to this practice as well as possible benefits to mood and alertness, though this does require some time and money to set up.
Improved night-time air circulation
Ranking: 4th
Intervention: Leaving a window or internal door open while sleeping.
Summary: There is reasonable evidence to suggest that high levels of carbon dioxide can accumulate overnight in a closed room and that this reduces sleep quality. Leaving a window open overnight is a simple and effective solution with minimal downsides.
Mindfulness-Based Stress Reduction (MBSR)
Ranking: 5th
Intervention: Completing an app-based mindfulness-based stress reduction course (MBSR) (e.g. Calm; The Mindfulness App)
Summary: Mindfulness-based stress reduction courses are associated with improved total sleep time and reduced sleep disturbance. MBSR is not targeted at sleep as an intervention and likely offers significant additional benefits.
Why sleep matters
The selection effects of choosing to read this article mean that you are likely already convinced that improving your sleep is a valuable use of your time. In case that is a poor assumption, this is a very brief argument in favour of the importance of sleep.
Sleep is fundamental to wellbeing
35% of American adults are estimated to sleep less than seven hours on average. This is considered sleep deprivation, with more than seven hours of sleep a night the consensus recommendation.
Sleep deprivation is linked to a higher risk of many (perhaps most[2]) negative health conditions, including hypertension, coronary heart disease, diabetes, and obesity. It has also been directly linked to lower reported quality of life and wellbeing.
This makes sleep one of the most effective interventions for improving other aspects of wellbeing. Though health issues like those above can in themselves reduce the quality of sleep, there seems to be a range of tractable ways in which to improve sleep regardless.
Modern living is not set up for ideal sleep
Perhaps some of the practices suggested here feel to you like an excessive intervention into the natural process of sleep, something that should not require supplements or training programmes. But in the excellent words of the writer Gwern Branwen, ‘I would point out to such readers that they are already profoundly tampering with their natural sleep cycle, and indeed, all of Western civilization is tampering with it’.
People tend to go to bed more than an hour earlier each night when taken away from any artificial light through the evening. Mobile phone use in the evening is a direct act of sabotage on the quality of your sleep.
EAs are smart people and have shown significant previous interest in sleep
There are eight previous articles on improving sleep on the Forum[3], as well as multiple high-quality posts on EA-related websites[4]. Taking the premise that effective altruists are generally smart people, the prevalent interest in sleep among the EA community suggests it is a smart decision to take sleep seriously.
Common (sense) interventions
The focus of this research is to explore the effectiveness of practices that are likely to be new to the majority of readers. Given this, we have omitted the exploration of a few common suggestions for improving sleep that are nevertheless worthy of some mention:
- Use earplugs or a white noise machine if you frequently notice ambient noise when trying to fall asleep.
- Install blackout blinds or wear an eye mask if you are often woken up early by ambient light.
- Choose a realistic time to get up each day and stick to it as much as possible. Trying to catch up on sleep over the weekends is ineffective and can be counter-productive in disrupting your circadian rhythm.
- Minimise the use of your bed for anything that isn’t sleeping.
Discussion of Primary Recommendations
Melatonin
Intervention: 0.3mg daily supplementation
Score: 5.95/10 (1st)
Melatonin is a hormone that triggers sleepiness and works to regulate sleep cycles. A small dose of melatonin taken daily (0.3mg, or 300mcg) produced a 4.8% increase in total sleep time (time spent in bed) and a 12.8% increase in sleep efficiency (the % of time spent actually asleep out of the time spent in bed) in this study.
Most commercial melatonin supplements come in significantly larger doses - often 3, 5 or even 10mg. While these doses also appear reasonably effective, there is a greater risk of negative side effects from regularly taking melatonin in these larger quantities.
These side effects are mostly mild (headaches, dizziness, or drowsiness the next day) but can be more significant (nausea, diarrhoea, or worsened depression). It is also worth being cautious about taking melatonin if you already take regular medication.
There is some evidence to suggest that melatonin supplementation can reduce blood pressure. It has also been linked with an improvement in symptoms for people with certain chronic health conditions, including cancer and endometriosis. However, it seems plausible that these improvements are a result of improved sleep rather than any additional effects of melatonin.
Once you’ve found a supplier of melatonin at the right dosage, this is a highly practical intervention. A year’s supply of melatonin should not cost more than $30 or so. Taking a capsule each night in the hour before bed requires little time or motivation.
CBT-I (Cognitive Behavioural Therapy for Insomnia)
Intervention: Completing a self-guided CBT-I course
Score: 5.78/10 (2nd)
CBT-I is a version of cognitive behavioural therapy specifically tailored for insomnia. Principally, it involves strict sleep hygiene coupled with sleep restriction, concepts that are nicely explained here. Previous research has found that CBT-I provided via individual or group therapy sessions can be more effective than prescription medication at treating insomnia, while also having far fewer notable side effects.
Though CBT-I is targeted at insomnia, the key principles of sleep restriction and strict sleep hygiene seem an improvement on common sleep behaviours. This makes CBT-I valuable to most people as a set of tools for improving sleep.
Our recommendation is based on the use of a CBT-I app, enabling access to the benefits of CBT-I without the cost or difficulty of finding a specialist practitioner. We found good evidence to suggest that six to seven weeks spent following an app-based CBT-I course produces significant improvements to sleep quality and quantity.
The best CBT-I apps currently available appear to be either Dozy, an EA-aligned CBT-I app available via beta testing, or CBT-I Coach, a partnership between the US Department of Veteran Affairs and the Stanford School of Medicine. As an alternative to using an app, Overcoming Insomnia is a CBT-I workbook produced by leading sleep medicine researcher, Colin Espie.
Light therapy
Intervention: Completing a self-guided CBT-I course
Score: 5.63/10 (3rd)
There is a significant range of research suggesting the benefits of increasing daytime and minimising night-time exposure to bright light. Most people working indoor jobs are exposed to only a small amount of bright light throughout the day. Bright light treatment generally aims for exposure to 10,000 lux, the equivalent of the light exposure outside on a day with light cloud, for two hours or more.
One study found that the average time spent in light over 1,000 lux (10 times less than the recommended level of ‘bright’ light) was 23% in ‘modern’ conditions vs. 71% in ‘natural’ outdoor living conditions. It seems reasonable to conclude that most people are now experiencing far less bright light than was normal for most of human history.
Exposure to bright morning light can reset the circadian rhythm. This in turn can reduce the time taken to fall asleep and minimise sleep disturbances through the night. The effects on total sleep time and sleep efficiency were generally moderate but consistently positive in the studies reviewed, with some studies showing improvements of more than 15% for patients with significant sleep issues.
Achieving exposure to 10,000 lux requires a moderate investment of time and money, but once a solution is found it can provide permanent benefit.
The simplest method is to purchase a SAD lamp that emits 10,000 lux and place this on your desk, maximising exposure while working. However, the light levels received from a SAD lamp can decrease significantly if placed too far from the face, while the lamp’s light offers minimal benefit when doing non-desk based activities.
The alternative is to install sufficient lighting in a room that the whole space is lit to 10,000 lux or more. This tends to involve buying 10-25 very bright lightbulbs which in combination produce the required brightness. Ben Kuhn and Eliezer Yudkowsky have each written good, practical guides for doing this.
Improved night-time air circulation
Intervention: Leaving a window or internal door open while sleeping
Score: 5.31/10 (4th)
Opening a window overnight can reduce CO2 levels in a bedroom by 60%. There is reasonable evidence to suggest that abnormally high levels of carbon dioxide cause significant decreases in sleep quality and cognitive performance the next day. Direct studies on the impact of improved air circulation by opening a window or internal door overnight are limited but suggestive of improvements in sleep quality.
Given the simplicity of leaving a window or door open, this intervention seems highly worthwhile. While an open window could make for a cold room, this too could be beneficial for sleep quality. An overly cold room also seems simple enough to fix with warmer bedding.
On top of this, improved overnight air circulation could plausibly reduce the accumulation of household air pollution, providing additional benefits to health and wellbeing.
Mindfulness (MBSR)
Intervention: Completing a self-guided MBSR programme
Score: 5.10/10 (5th)
Mindfulness-based stress reduction combines practising mindfulness meditation, non-judgmental awareness, and exploration of the feelings and sensations associated with stressful events. A six-week MBSR course produced a 37% improvement in Pittsburgh Sleep Quality Index scores, an aggregated measure of sleep quality and quantity. While app-based therapy appears less effective than this, it is still likely of significant benefit. Specific research into the effects of app-based MBSR on sleep is limited, but this randomised control trial found a significant decrease in sleep disturbance for users of the meditation app Calm.
Given that this and other research has found significant benefits from mindfulness training for numerous aspects of wellbeing, MBSR appears a valuable intervention. In some cases, mindfulness training can make individuals more aware of negative behaviours and thought processes without providing relief, though this appears to be an uncommon outcome.
Apps tailored to improving sleep do not appear common. Two suggestions based on a limited review of available solutions are Calm and The Mindfulness App.
Secondary Recommendations
The following is a summary of the other interventions explored in-depth that did not score as high in our assessment.
Mattresses
Intervention: Changing to a medium-firm mattress
Score: 5.05/10 (6th)
Replacing current bedding with a new, medium-firm mattress appears to produce a 5-6% improvement in sleep quality and efficiency. While individual preferences may differ, the majority of studies that we analysed concluded that a medium-firm mattress was the optimal type for maximising sleep quality.
Mattresses, however, are a significant investment that may not be practical or worthwhile for many given the only moderate improvement in sleep quality. Additionally, studies tended to test subjects who were previously sleeping on mattresses several years old. Given this, we can reasonably expect a diminished effect for people with more recently purchased bedding.
We make no attempt to recommend specific mattresses given the large differences in price and larger amounts of marketing involved in their sale.
Caffeine
Intervention: Eliminating caffeine consumption from the late afternoon onwards
Score: 4.95/10 (7th)
Caffeine is a commonly known and consumed stimulant. That caffeine can make it more difficult to fall asleep is fairly obvious. However, regularly high consumption of caffeine can also have a significant impact on sleep quality.
The impact of caffeine on sleep can be avoided by limiting consumption to the first half of the day. Individuals’ speed of processing caffeine varies significantly but it is common for it to still have notable effects up to 10 hours after consumption.
At a minimum, avoiding caffeine consumption within the six hours prior to sleeping seems an easy and valuable intervention. Adjusting the results of this study to the caffeine content of a standard double-shot coffee, we estimate a 3% reduction in sleep time and sleep quality from drinking a coffee six hours in advance of sleep.
Though caffeine consumption has a significant effect and strong evidence base, we expect that avoiding caffeine later in the day is largely common knowledge. Given this, people who currently drink coffee in the evening are likely doing so for benefits that they weigh higher than a small increase in sleep quality (such as increased alertness for evening work), making this a less valuable recommendation.
Magnesium
Intervention: Taking a 300mg magnesium supplement daily
Score: 4.76/10 (8th)
Around half of Americans likely consume less than the recommended levels of magnesium, while some studies have suggested that recommended levels are significantly lower than the optimum daily magnesium intake.
While the quality of evidence is low, with no known method of causation, magnesium supplementation is associated with improved sleep efficiency and total sleep time.
Most multivitamins only contain a modest amount of magnesium[5] so we recommend taking a specific, 300-375mg magnesium supplement to test for any noticeable benefit to your sleep. However, magnesium supplementation can have significant side effects, particularly for people taking other medication, so it is important to note possible issues and stop taking supplementary magnesium should these occur.
Cold lighting
Intervention: Installing blue-enriched lighting to your workspace
Score: 4.53/10 (9th)
While lighting can come in a wide range of brightness, it also ranges widely in colour temperature. Blue-enriched (cold) lighting can improve daytime alertness and bring a modest benefit to sleep quality but is difficult to find commercially.
In our brief search, we found these household lights at 6,000K as the coolest option available. However, the blue-enriched lights used in the study referenced above were 17,000K, meaning that the benefits of commercially available cold lighting are likely to be significantly lower than those produced in research.
Given the greater evidence base and strength of effect for increasing the brightness of household lighting, we feel that this is a more worthwhile intervention than installing colder lighting.
Morning exercise
Intervention: Shifting exercise from evening to morning
Score: 4.43/10 (10th)
The positive effect of regular exercise on sleep quality is well-known. However, the timing of exercise during the day could play a significant mediating role in increasing or decreasing the beneficial effects of exercise on sleep.
For people accustomed to exercising in the evening, shifting their practice to the morning could increase sleep quality while reducing sleep disturbance and the time taken to fall asleep. However, these effects were relatively modest in the research we found and evidence on the topic is thin.
With the constraints of coordinating work, family, and social schedules, we expect that shifting exercise time will be relatively difficult for many people. Feasibly, it could even result in reduced sleep hours if you start waking up earlier to fit in exercise in the morning.
Houseplants
(Note: see this comment for why the estimate given below is likely a significant overestimate of the potential effect of houseplants on bedroom CO2)
Intervention: Buying multiple succulent houseplants for your bedroom
Score: 3.94/10 (11th)
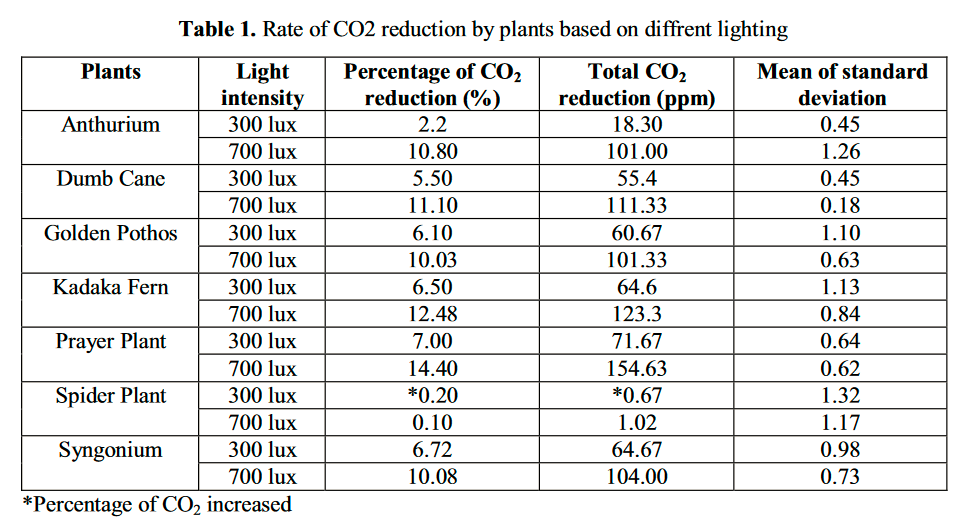
As an alternative to opening a window, there is some evidence that some houseplants can produce a notable reduction in CO2 levels in a room. In particular, certain plants that store CO2 at night to then use for photosynthesis during the day (a process known as crassulacean acid metabolism [CAM]) appear particularly effective at reducing night-time CO2 levels.
While there has been little research into this area, one study found several common houseplants reduced CO2 concentration in a room by 15-20%. It seems reasonable to assume that placing several houseplants in a room would significantly increase this effect, though likely with diminishing returns.
A study conducted by NASA into the effectiveness of houseplants at removing a range of air pollutants (to then use them on the ISS) found that Variegated Snake Plants and English Ivy were particularly promising.
We leave the decision of whether to create a small indoor forest in your bedroom in your hands but note that this is unlikely to be more effective at reducing CO2 concentration than simply opening a window.
Summary
This research forms an attempt to find the most effective ways an individual can improve their sleep, with a focus on suggestions that readers are less likely to have previous knowledge of. The methods used are rough and a work in progress, forming the basis of a larger project researching the most effective ways people can improve their wellbeing.
Our principal recommendations for improving sleep quality are (in order):
- Melatonin supplements: 0.3mg (300mcg) daily taken two hours before bed.
- CBT-I: a six-to-seven-week, self-guided course in cognitive behavioural therapy for insomnia, accessed through an app.
- Light therapy: greatly increasing exposure to bright light during the day, either through building a lumenator or purchasing a SAD lamp.
- Improved night-time air circulation: opening a window to reduce overnight CO2 accumulation.
- Mindfulness-based stress reduction: mindfulness training through an app with a focus on sleep.
Thank you to everyone who has previously written about improving sleep here on the Forum[3:1] and on other EA-aligned sites.[4:1] We hope that this research has been useful and that you’ll consider experimenting with our recommendations!
Note: We are currently running a 5-minute survey evaluating our work which we'd greatly appreciate you filling out!
The model used for this research is a rough one, loosely based on the weighted factor models used by the Charity Entrepreneurship team. A model like this allows for the inclusion of a wider range of subjective and objective measures, combining practical aspects of an intervention with evidence of its effectiveness. Results should not be taken as definitive, acting instead as a guide for updating knowledge in a positive or negative direction. As the wider project grows, this model will likely be further developed. The results posted here will be updated accordingly. ↩︎
We were going to establish the accuracy of this claim but decided it would be more worthwhile to get some extra sleep instead [it was]. ↩︎
Thank you to everyone who has previously written about sleep on the Forum. The following is a (hopefully!) comprehensive directory of previous articles on the topic published on the Forum (in order of karma): Burnout – what it is and how to treat it: Sleep [Elizabeth]; Insomnia with an EA lens: Bigger than malaria? [samstowers]; Insomnia: A promising cure [Halstead]; On Sleep Procrastination: Going to Bed at a Reasonable Hour [emily.fan]; Things I recommend you buy and use: Health/ Sleep [BenSchifman] Should we consider the sleep loss epidemic an urgent global issue? [orenmn]; Instructions on potential insomnia cure [Halstead]. ↩︎ ↩︎
Other great EA-adjacent articles: How to improve your sleep [Lynette Bye]; Behavioural treatments for insomnia [Luke Muehlhauser]; Melatonin: Much more than you wanted to know [Scott Alexander] ↩︎ ↩︎ ↩︎
Magnesium content in the first 5 multivitamins I found through a quick Google search: Vitabiotics Wellman Max [60mg]; Holland & Barrett Ultra Man Multivitamin 30 Caplets [125mg]; Boots A-Z 180 Tablets [60mg]; Centrum Advance 50+ [100mg]; Vitabiotics Wellwoman Max [100mg]. ↩︎
MichaelPlant @ 2021-11-18T10:48 (+43)
While I am as much a fan of wellbeing research as the next fellow - indeed, probably a much bigger fan - I have to say I found the methodology and conclusions of this research rather confusing.
If I were approaching this topic, I would have (1) done a review of the existing literature to find out what people thought was effective and what the possible interventions were, then (2) tried to assess the options in terms of (a) a comparable metric of effectiveness and (b) cost, so readers could think about what would do the most for them at the least effort.
As it is, this research seems to have missed out many of the standard pieces of advice like avoiding alcohol, napping after 3pm, having a large meal before bed, or having a sleep routine. The author doesn't mention having looked at the existing literature, but does note that other EAs have mentioned sleep. I don't mean to single out the OP, but I do want to deride the myopic and self-referential tendency among effective altruists in general to overlook work done outside effective altruism. Lots of good has happened 'out there' and we ignore it at our peril.
What I found least satisfying about this research was how this (partial list of) interventions were assessed. As far as I can see, the 'weighted-factor model' involved assigning unexplained subjective numbers to various seemingly-arbitrarily chosen properties, then assigning a seemingly-arbitrary weight to each factor to aggregate them. * I am reminded of "Garbage-In-Garbage-Out" concept in computer science where nonsense inputs products nonsense outputs. As a reader, I have no idea how to interpret the rankings or numbers - what does it mean that melatonin gets "5.95/10" or that CBT-I gets "5.78"? - or how much to update off them. The results are basically uninterpretable.
I would strongly recommend that the OP heavily revise their methods and the presentation of their research for any further work. The main thing would be to present the results of the interventions in a standardised metric, e.g. total sleep time, or standard deviations of something, so readers can make a comparison themselves, then make comments on cost and, if necessary research quality. I am happy to provide advice if that's helpeful.
*I recognise the weighted-factor model is something Charity Entrepreneurship use. I have raised it with them several times that, for the reasons given, I find this approach hard to follow or justify and thus questionably useful.
Ben Williamson @ 2021-11-18T12:16 (+11)
Thank you for the feedback!
There's a few points you make that I feel are important to clarify but I want to first acknowledge that the format and presentation of the research is a work in progress and could definitely be improved. In particular, I can agree that the "5.95/10" numbers aren't particularly useful given the lack of any context/ scale.
To respond quickly to a few specific points:
1) This research was overwhelmingly based on the existing literature. I chose not to include a reference list or in-text citations to maximise the readability of the text but perhaps this was an error.
2) The interventions' strength of effect, which accounts for about 40% of the score, is an average of improvements in sleep efficiency and total sleep time found in the literature I reviewed. In hindsight, I think it could have been better to highlight these findings on their own in the text and may add them in.
3) The focus of this research was to explore interventions that the reader is less likely to have heard of previously. I assumed that ideas like avoiding alcohol and late naps are things that nearly all readers would already know. On that basis, I felt that highlighting them in an article like this is unlikely to produce any change in behaviour, though I can see now the potential usefulness of presenting the size of effect.
4) I think an article like this recommending low-cost, personal interventions can reasonably have a different approach and level of rigour to one recommending charitable interventions and/or shifting large sums of money. A weighted factor model may not be the best way to frame this research but I think additional considerations like the potential risks and additional benefits of a recommendation are important and necessary to highlight.
These points make me realise that a more explicit description of the methods used and the literature reviewed would be valuable for future posts, rather than linking to them in out-of-text docs or leaving them out for a marginal improvement to the conciseness of the text.
This is the first post intended in a series and I expect to revise and improve the methods involved with each post and certainly the feedback I get on posts helps to direct that process. As a first attempt, some of the process was not as rigorous as it could or perhaps should be. In part, this is a relatively time-limited project for now (~3 months) so I am sacrificing some potential added depth in each post for the ability to cover more topics.
On a final note, I have immense respect and appreciation for the work of HLI and so really appreciate the feedback from someone who does wellbeing research at a much higher level!
MichaelPlant @ 2021-11-19T11:36 (+19)
Hello Ben!
Good to know this was based on existing literature. In most cases, it helps to show the reader you know that literature, to outline what it is, and then go on say what your new contribution is. Like I say, you missed a few of the obvious things, which is unfortunate. A piece of "what works for X" should, I say, include the things that work for X, then perhaps go on to flag which of these are likely to be a surprise, rather than assuming on the reader's behalf what they will already know. If you are going to have a piece on "what works for X that might but that might surprise you" you should at least clearly flag that, and then point to something such as "standard guidance on X".
Re strength of interventions being "40%" that still seems a confused way of presenting the information. 40% of what? Of a maximum score? A maximum score of what? Of cost-effectiveness? Well, why not just present the effectiveness numbers and divide them by the costs then?
I agree that this sort of thing can have a lower level of rigour but I stand by my concern that the method you use is so puzzling it's questionably useful at all. You gathered quite a bit of relevant info, but I think you presented it in a less-than-ideal way. Here, simpler would have been better: I'd have preferred a post that just said "here's a list of evidence-based ways to improve sleep" and then listed them and provided a brief discussion on each. That seems the way to go unless you have the data and time to do a quantitative (cost-)effectiveness analysis.
Glad you think we (at HLI) do good work. Like I see, feel free to reach out if you want to chat about research methods etc.! You can get me at michael@happierlivesinstitute.org
David_Moss @ 2021-11-15T20:07 (+24)
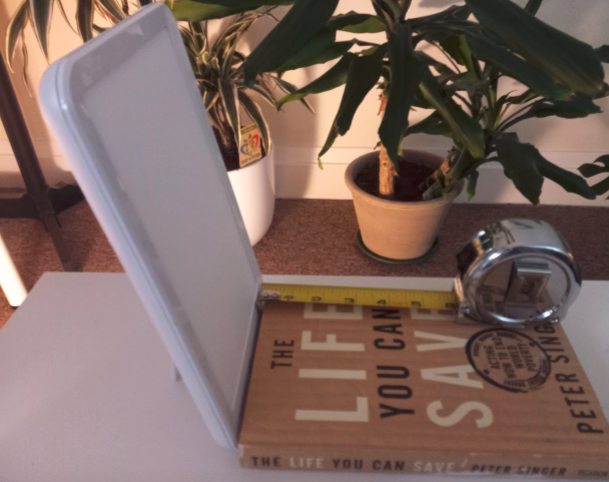
The simplest method is to purchase a SAD lamp that emits 10,000 lux and place this on your desk, maximising exposure while working. However, the light levels received from a SAD lamp can decrease significantly if placed too far from the face, while the lamp’s light offers minimal benefit when doing non-desk based activities.
This really bears emphasising, since most SAD lamps (accurately) marketed as "10,000 lux" are 10,000 lux only at distances much shorter than most people might expect or might be able to achieve with their desk setup (see Scott Siskind's Lorien Psychiatry page on this).
I was recently shopping for some new SAD lamps and most were 10,000lux at around 15cm (6 inches). See below using a copy of The Life You Can Save as reference. This suggests your eyes would need to be this close for the lamp to count as "10,000 lux". I also have a larger, more expensive lamp which gives about 7cm (2.7inches) more wiggle room. One of the most commonly available powerful lamps I've found available in the UK would allow your eyes to be about 3 inches back from the edge of the book.
Ben Williamson @ 2021-11-16T10:23 (+4)
Thanks for highlighting this! The image really makes apparent the issue in a much more obvious way. It's a shame there aren't SAD lamps designed to offset this, at least from what I've seen (e.g. by producing more than 10k lux to begin with). This issue definitely makes the construction of a whole-room lighting setup a more valuable solution.
Lukas Trötzmüller @ 2021-11-16T17:57 (+2)
Relevant work demonstrating bright full-room lighting as an alternative to an SAD lamp: https://forum.effectivealtruism.org/posts/bwhDhZQvbEcG4FEb8/preprint-is-out-100-000-lumens-to-treat-seasonal-affective
David_Moss @ 2021-11-17T12:06 (+3)
Thanks! It's cool they have done a study on the 'full-room' approach.
I think full-room approaches are worth people looking into, but it's worth noting that they are usually less bright than using SAD lamps (and this goes for the setup described in the pre-print too). As noted, in the pre-print, they put out more light, but because you are usually much further away from the lightbulbs distributed around the room than you would be from a light box on your desk, the mean illuminance at eye level was 1433-1829 lux. By comparison, I have three of the light boxes photographed above on my desk (quite a distance, more than arm's length), and they're each around 5000-7680 lux at eye level. Of course, it's possible to get much larger amounts of light from either approach.
As the pre-print notes, natural summer sunlight exposure has a few characteristics that might be advantageous over typical light therapy, i) much brighter, ii) covers the whole visual field, iii) exposure for many hours of the day, not just a short period in the morning.
I agree that (ii) might be important and potentially a significant advantage of the full room approach over light boxes. IME, one significant difficulty with getting a large amount of light from a small/concentrated source (such as a light box) is that it's subjectively very uncomfortable. Daylight, conversely, usually provides much more light but without the uncomfortable glare of having a single, very bright light in front of you. Ironically, when I tried setting up large number of bright lightbulbs around my room previously, they are actually less comfortable than light boxes, because without being fully covered by diffusers (as SAD lamps usually are, but which reduces the brightness a lot), the single points of very bright light coming from the bulbs were more unpleasant than the light boxes. Of course, there are very many different ways you could set these up in a room, including having more bulbs, but all with diffusers, so YMMV.
The authors are also right that being able to just sit in a bright room and move around freely within in might be a significant advantage (or a practical necessity) for many people. This isn't really a factor for me, and I'd imagine many EAs, since I am at my desk most hours and so can be exposed to my SAD lamps pretty easily.
I'm also uncertain about how less bright light spread roughly evenly across the day compares to the typical very bright dose of light first thing in the morning. It seems possible that the brighter light first thing in the morning is superior for circadian rhythm entrainment (and so improving your sleep), though it is also possible that less bright light throughout more of the day is superior (perhaps mediated by higher volume), or that this is superior for SAD, but not for circadian rhythm per se. I'd be interested if anyone knows any high quality studies that tease this apart. I often wonder, for myself, whether it would be better to have a high light dose only relatively early (and then cut it off) or to maintain a high light dose throughout most of the day.
RayTaylor @ 2022-01-10T18:43 (+1)
I find the ReTimer glasses much easier to use, £120 and portable for travelling.
Lakin @ 2021-11-16T01:21 (+13)
I'm surprised you haven't mentioned temperature. E.g. buying a chilipad brought down my night-time insomnia by ~80%. (And I live in the northeast, too!)
Recently I've moved my bed directly next to my air conditioner, which has been great
Lakin @ 2021-11-16T01:19 (+11)
Have you investigated the effect of night-time darkness?
https://www.pnas.org/content/116/24/12019
Also of blocking blue/green light? Though there's only a handful of studies
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7229994/ - found a 58% increase in night-time melatonin (blocking just blue, though separately it might do well to block green too)
I think I have some more notes lying around somewhere if you need them
Ben Williamson @ 2021-11-16T10:32 (+1)
Thanks for the suggestions! I think I may come back to this and expand the number of interventions I've reviewed and these are valuable suggestions that could well be worth promoting.
Temperature and daytime sunlight are both somewhat mentioned in the article already but may be worthy of their own specific sections. I'd expect the benefits of daytime sunlight to roughly equal light exposure + Vitamin D. Given that, I think light therapy probably covers the majority of the positive effect but this likely warrants more specific research.
With the larger project I'm working on in mind, there's a balance to be struck between research depth on a certain topic and breadth in the number of topics that I cover over the next few months, so there's definitely more depth that could be added to an article like this to improve it.
Lakin @ 2021-11-17T15:32 (+6)
Yeah, time constraints as expected. I think I found the title of this post a bit strong then.
Also, I would be surprised if light exposure + Vitamin D approximates daytime sunlight at more than 50% effect.
Ben Williamson @ 2021-11-17T16:23 (+1)
I think that's a fair point about the title and have changed it in light of that. I'm curious as to what you'd expect the other 50% of effect to come from? (no snarkiness intended)
Lakin @ 2021-11-19T02:20 (+4)
On the vitamin D side: In I'm pretty skeptical of reductionist viewpoints in general such as here, ~"the single compound of 'vitamin D' placed into supplements has nearly the same effect as broad-spectrum UV on skin affects the body". I wouldn't be surprised if broad-spectrum UV had plenty of other effects that we have no idea how to look for, or for example if "UV → {this specific compound that is put in supplements}" is a poor approximation (maybe broad-spectrum UV causes the production of plenty of compounds that are also great, and we're only inclined to supplement one).
E.g. Vitamin D2 could be an easy way to go wrong here (I've only ever criticism about the effectiveness of D2). If Vitamin D supplementation works at all, I would bet on D3, but I haven't seen you make this distinction.
Overall I think this is pretty complex to make such general reductionist prescriptions (e.g. take 'Vitamin D3, X IUs everyday in the morning…") unfortunately.
((Also, we might live in a world where the supplement Vitamin D3 is fairly ineffective, but it still causes the blood biomarker to increase, confounding all studies everywhere.))
I used to supplement Vitamin D3 for a few years, but I stopped when I heard about all of these subtle ways that it could be ineffective (or harmful). Instead, I took more walks outside, and I took my shirt off while in sunlight more often. I have also noticed I feel much better this way, quite calmer, and I suspect quite a bit more productive on these days, and I've never gotten that from a supplement.
On the light exposure side: 10,000 lux is still an order of magnitude less than sunlight! Also, I doubt these lamps emit any UV, and I expect that a lot of the effect of sunlight comes from UV and that which we cannot see.
emily.fan @ 2021-11-21T04:11 (+1)
Just wanted to +1 blue blocking glasses.
Manon Gouiran @ 2022-04-05T11:07 (+7)
Effective Self-Help is looking for feedback! Hi everyone, we're looking to evaluate our work up to now researching the most effective wellbeing and productivity interventions. We'd really appreciate you filling out this 5-10 minute evaluation survey which will help us figure out how we can be of most help to the EA community.
You don't need to have read any of our reports up to now to fill out the survey so we'd love to hear your thoughts, even if you've never heard of us before! Thanks in advance for your help!
David_Moss @ 2021-11-17T12:56 (+7)
Regarding magnesium, the specific supplement you happened to link to was magnesium oxide. There's some evidence that magnesium oxide is less bioavailable than other forms of magnesium (1,2,3) It's true that magnesium oxide is cheaper, but magnesium citrate is still exceptionally cheap (a few pence per dose). So, even if you are uncertain about the benefits of other forms over oxide, I think it's still probably reasonable to err in favour of these other forms.
I think it's also worth thinking about glycine. There are a few papers suggesting that glycine improves sleep quality (4, 5, 6, 7). You could also take magnesium bisglycinate, which contains both magnesium and glycine, but aside from convenience of only having to take one thing, I don't see any advantage to doing that rather than just dosing them separately.
emily.fan @ 2021-11-21T04:12 (+1)
Agree that the quality of magnesium matters!
https://www.youtube.com/watch?v=XfeiBd8h6Xw https://www.youtube.com/watch?v=jTiXVGwZLO4
Lakin @ 2021-11-21T14:36 (+6)
I think it's pretty weird that Melatonin is #1 in your list. I think it's weird to suggest exogenous supplementation of something like that without an explanation of why melatonin is low to begin with. The efficient market hypothesis, but applied to your own biochemistry. Chesterton's fence, etc.
The body isn't a machine- as if you can just give it the right amounts of the right compounds and it will perform optimally.
Lakin @ 2021-11-16T01:22 (+6)
What about the effects of daytime sunlight on sleep? (I would be hesitant about confounding sunlight exposure with vitamin D supplementation, I think it's unlikely that they're equivalent.)
RayTaylor @ 2022-01-10T18:45 (+1)
Being outside daytime and keeping the bedroom area for nighttime use are both known to be helpful which is why they are part of CBT sleep hygiene.
You're right that it's not linked to vitamin D, which is via the skin not the eye/pineal/melatonin circuit.
Thomas Kwa @ 2021-11-15T21:00 (+6)
Melatonin supplements: 0.3mg (300mcg) daily taken shortly before bed.
What's the reasoning for taking it shortly before bed? I've heard that the default time to take melatonin should be a couple of hours before bed, except to treat delayed or advanced sleep phase.
Ben Williamson @ 2021-11-16T10:20 (+1)
Thanks for flagging this! I'm going to edit it and clarify as 'shortly' is not a very specific recommendation. I've seen recommendations ranging from 30 minutes to 3 hours, with 1-2 hours being most common, so it's not exactly clear when is most effective. Earlier doses seem to cause some people to wake abnormally early.
I'll change this to 2 hours as that's what was used in the literature cited.
Yonatan Cale @ 2021-11-17T18:41 (+4)
>2 hours as that's what was used in the literature cited
Are you talking about that single study?
My current prior is that the optimal time for melatonin before bed changes between people, and I suggest that my friends experiment with it in nights that aren't so important first, in case it doesn't work well. [The reason is that I'm confused about Scott's recommendation to take it mid-day or to take it just-before-sleep]
Regarding the recommendations you saw - I'd want to dig into "what are they based on". The article Thomas linked to gives the best review I've seen about what we know about Melatonin (as Scott Alexander often does when he summarizes scientific topics)
Adding: The same article recommends a supplier, and I also check suppliers here.
And while I'm at it, gwern also writes quality in depth reviews, including about melatonin
Ben Williamson @ 2021-11-17T20:31 (+2)
Both the Slate Star Codex and Gwern articles are great and helped inform the article! (I think both are linked at points in the text)
And yes, 2 hours is the timing used in the Zhdanova study. I couldn't find a clear consensus on any particular timing so I have chosen this without doing significant further research. I completely agree with you that experimenting with the timing of it seems ideal.
David_Moss @ 2022-06-16T11:44 (+3)
one study found several common houseplants reduced CO2 concentration in a room by 15-20%. It seems reasonable to assume that placing several houseplants in a room would significantly increase this effect, though likely with diminishing returns.
Unfortunately, I am quite a bit less optimistic about this. (Caveat: I only looked into this very briefly)
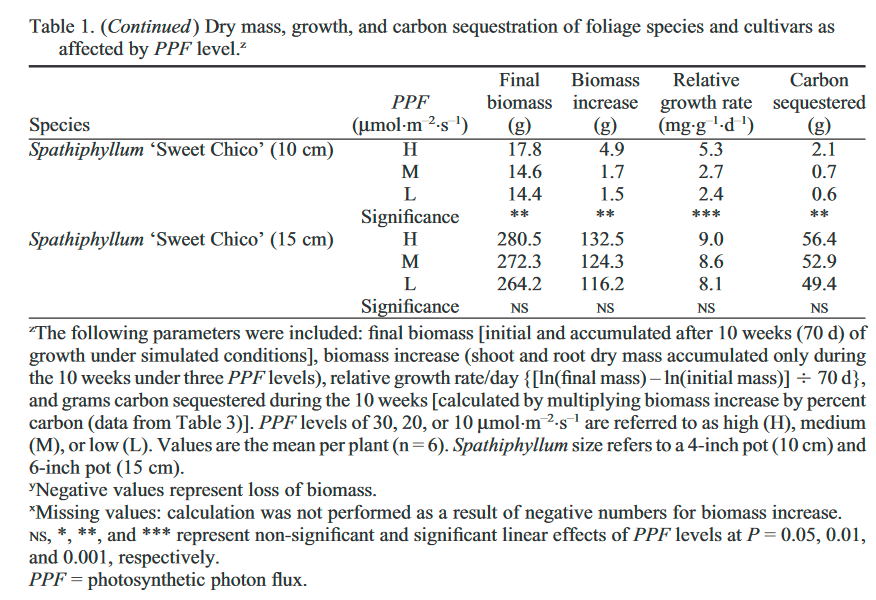
From quickly looking at the conference paper you cite, it seemed that the plants were in 1 cubic meter chambers and reduced CO2 by ~50-100ppm for the most part (~5-12% reduction) based on table 1.
But bedrooms are generally a lot larger and contain at least one human breathing out carbon dioxide into them. This paper suggests that since humans breathe out about 300g per day, ~400 plants, in good conditions, would be needed to offset this. Naturally only a portion of that 300g is breathed out into one's bedroom at night, but it still seems like one might need ~100 plants for one person in a room, and one would need to ensure that these are plants which take up CO2 at night, rather than exhaling it at night.
Ben Williamson @ 2022-06-16T19:44 (+2)
Thanks for flagging this. It does seem from this that I've oversold the potential value quite significantly! I'll add a note to the section to flag this comment and that this doesn't appear to be as helpful as hoped.
David_Moss @ 2022-06-16T20:28 (+2)
Thanks! It's a pity, because I'm a big fan of house plants, and the heavy blackout blinds I use prevent getting fresh air via windows at night, so this would have been convenient if true.
Jeff Kaufman @ 2022-06-16T12:31 (+1)
If you want to absorb 300g/day of CO2 you need the plants to grow by ~300g/day. Which is a lot!
(It's only rough: 300g of CO2 is 12/(12+2*18) carbon, but when absorbing carbon plants also take in water with goes the other way)
David_Moss @ 2022-06-16T13:26 (+5)
I think (though, again, I only read it quickly) the paper includes estimates for both carbon sequestered and biomass growth for the plants.
I believe the plant which they used as the reference for that rough figure above increased in biomass by 132.5g but sequestered 56.4g carbon over several weeks, and the 0.8g carbon fixed per day comes from that latter figure.
Xing Shi Cai @ 2022-06-08T06:38 (+3)
I had trouble of having enough sleep lately. Often I woke up early and could not go back to sleep again. Last night I took 0.3mg melatonin and this morning I missed my alarm clock and slept for 9 hours straight! 😲
It may be because that I slept for only 6 hours the night before, but it has never happened before that I would not wake up by alarm clocks. But this is a promising beginning.
RayTaylor @ 2022-01-10T18:35 (+3)
Thanks for opening this topic. It's important to realise there are different kinds of sleep problem, so different people will need different solutions:
- sleep onset
(which tends to be due to stimulation too late at night; CBT sleep hygiene works well for this, if done diligently, and limiting coffee etc) - early morning waking
(which tends to be due to stress-anxiety-depression or large amounts of alcohol) - low sleep quality
(which can be due to a range of things but alcohol and the wrong medication is a classic cause; Mirtazapine is popular, but has long term dangers like weight gain)
In the UK, melatonin* is no longer available without prescription, only 5-HTP, which is a precursor. Is this because people tended to take dangerously large doses of melatonin? (Precursors tend to be safer, because the body can convert the amount it needs, at the right time.)
Generally fresh air is a good thing but there are caveats especially during a pandemic winter. If you pull in too much very cold air (with low absolute humidity) you can quickly go below 40% RH which is bad for the protective mucus layer of the lung & airways, and the glycans+non-IgG antibodies which are important for innate immunity.
What makes you think slightly lower CO2 or higher O2 levels are good for sleep? Isn't the converse equally or more likely? (If not, people who live in mountain areas are in trouble! And I sleep really well in the mountains.) I have noticed that people in higher CO2 environments seem drowsy. Of course, this too may not correlate with good quality sleep!
Are you defining good sleep just by duration? For more on this, search < sleep architecture CBT >
On the SAD lighting, many people find the room lighting or boxes impractical. Much easierfor some is a visor or glasses which can be worn while preparing breakfast etc. I've been happy with an Australian brand (www.re-timer.com/the-science/research) but there are others that may look cooler!
* https://www.webmd.com/sleep-disorders/news/20181112/as-melatonin-use-rises-so-do-safety-concerns
https://alaskaregional.com/blog/entry/4-reasons-to-be-cautious-about-melatonin
Chriswaterguy @ 2022-06-12T23:58 (+1)
5-HTP is a precursor to serotonin, which is a precursor to melatonin. I imagine that this would have a much slower and less predictable effect, less suitable for helping to go to sleep in a particular time range.
I share the concerns about possible overuse of melatonin, though I've found out helpful at times. I try to adjust light exposure (morning and night) as a higher priority than melatonin.
I may also go back to using low dose melatonin, though, as it's been helpful in the past and may be needed in modern technological society.
Lakin @ 2021-11-16T01:23 (+3)
recording oneself sleeping for snoring/sleep apnea seems huge.
(sorry for the comment spam. I have lots more ideas too, feel free to email me, https://chrislakin.com/now.)
Yonatan Cale @ 2021-11-17T18:50 (+2)
I have a friend who did this and discovered they stop breathing multiple times per night. Later they ordered an OuraRing and confirmed this.
Easy way to check: The Sleep As Android app has a snoring-recording feature.
Lakin @ 2021-11-19T02:21 (+1)
ty for the app! do you know of one for iOS?
Dave Cortright @ 2022-04-10T21:07 (+2)
Thanks for taking the initiative to publish this. I offer these resources
- A good all-around guide from The Blue Zones
- Humans may be hard-wired for segmented sleep
- If you are getting poor sleep, you may be lonely
Johann Hari touches on this last one in his excellent book, Lost Connections:
Anywhere in the world where people describe being lonely, they will also—throughout their sleep—experience more of something called ‘micro-awakenings.’ These are small moments you won’t recall when you wake up, but in which you rise a little from your slumber. All other social animals do the same thing when they’re isolated too. The best theory is that you don’t feel safe going to sleep when you’re lonely, because early humans literally weren’t safe if they were sleeping apart from the tribe. You know nobody’s got your back—so your brain won’t let you go into full sleep mode. Measuring these ‘micro-awakenings’ is a good way of measuring loneliness… [A researcher studying the Hutterites in the American Dakotas found] they had barely any. The [Hutterite] community showed the lowest level of loneliness that [the researcher had] seen anywhere in the world. It really stunned [him].
michaelchen @ 2021-11-18T14:45 (+2)
After reading this post, I'll try out the Dozy app for CBT-I, even though I don't really have insomnia per se.
For bright light therapy, it's confusing to me why exposure to daylight isn't more often as a solution. Would it make sense to say that, if you live in a reasonably sunny place and have time to spend time in the daylight, then you should consider just spending more time in the daylight, not only light boxes? Sunlight is often a lot brighter than the 10,000 lux of a light box, and it fills the entire visual field.
RayTaylor @ 2022-01-11T00:02 (+2)
Yes that would be better.
(But be careful of sunburn, especially in the tropics and at altitude!)
Ramiro @ 2021-11-17T15:33 (+2)
Thank you so much for this post - great work.
Your discussion of light therapy made me wonder about the effects of outdoor activities on sleep (and maybe other wellbeing dimensions). Any possibility you're going to analyse it in the future?
Ben Williamson @ 2021-11-17T20:32 (+2)
Thank you! I'm definitely interested in potential additional benefits from being outside. I have a rough intention to do a more in-depth analysis of bright light exposure and its full range of wellbeing benefits at some point. I think this, alongside vitamin D, approximates a good amount of the benefit of being outdoors.
Chriswaterguy @ 2022-06-13T00:02 (+2)
It's worth noting that being outside in sunshine gives much more intense light exposure than any mainstream SAD treatment. (My personal experience is that it can give a large boost in alertness, and probably helps my sleep significantly. But I'm in Sydney – I can't speak for northern Europe or Canada.)
Ben Williamson @ 2022-06-16T19:33 (+1)
This makes sense and seems pretty plausible. Can speak to personal experience of the intensity of the sun in Australia!
MaxG @ 2021-11-16T13:09 (+2)
About mindfulness: I have been meditating daily for a few years and have tried a bunch of different apps.
The one I can recommend the most and use personally is Waking Up (https://wakingup.com/). Not only is it IMO the best app for mindfulness meditation, but they are also EA aligned. They signed the GWWC pledge and were among the first batch of companies to do so. If you can't afford the subscription, you can email them and get it for free.
Would be curious to hear what experiences others have had with meditation apps.
Ben Williamson @ 2021-11-17T10:52 (+4)
+1 for the Waking Up recommendation. Definitely the best meditation app I've used, with a lot of interesting content around what it means to live well more generally, plus the series with Will MacAskill on EA. I'm planning to do a proper write-up of meditation and mindfulness benefits and options in the near future.
Chriswaterguy @ 2022-06-12T23:41 (+3)
My favourite is Ten Percent Happier – it's very accessible and it has a lot of meditations and teachings by Joseph Goldstein, who also appears in the lectures in Waking Up. I've also found some value from Sam Harris's meditations, especially the early ones he released long before the app. Ten Percent Happier don't have the free option AFAIK, but they do have an 8-part free intro. And they have significant discounts at times through the year.
Bryan Hanlon @ 2021-11-18T01:27 (+2)
I agree on the Waking Up app. I have tried Headspace, Calm and Waking Up and found Waking Up to be the best choice for me. Specifically, the Theory section has been helpful to me as a beginner trying to learn about meditation. I also appreciate that it lacks some feature that I find corny in other apps, such as celebrity cameos. However, it may not be best people who don’t care for Sam Harris due to his various political positions, or those who do like him, but associate his voice with his podcast.
MaxG @ 2021-11-16T10:58 (+2)
Thanks for writing this up, this is a good list. I used to struggle with getting to sleep for years, taking 1-2 hours to fall asleep on most days. To everybody with sleep problems, I want to encourage you to experiment with some of the above mentioned interventions. It is possible to improve your sleep. I have tried most of the things on this list and have had great success.
Just as an anecdotal data point:
One of the problems I had specifically was just going to bed way too late because I didn't get tired earlier than midnight. Being a night-owl isn't a problem per se, but honestly the world is more tailored to benefit early-risers. It sucks to have to cut short on your sleep because you have a mandatory Uni course at 08:00.
For a few months I have been taking this 300mcg melatonin every day exactly at 17:00 after reading this article. It reliably makes me tired at 22:00-23:00 and I fall asleep astoundingly quickly if I go to bed in that time range. Something interesting I noticed is that when I go to bed later than that time, e.g. at 02:00, my tiredness is gone again and I find it much harder to fall asleep. Not sure if this is just placebo. Keep in mind that this will vary from person to person and my experience is probably different from yours. Also I do at least 5 other things to sleep better so there are many confounders and I don't know how much to attribute to using melatonin. Just experiment and see what works for you.
(I'm not a doctor and this is not medical advice)
Derek @ 2021-11-19T18:37 (+1)
Is the CO2 accumulation entirely due to human (or I suppose animal) respiration? So it will typically be worse in small houses with lots of people (holding other factors, like ventilation, constant)?
In a modern house, with no open fires, lead paint etc, what "household air pollution" might there be?
RayTaylor @ 2022-01-10T23:51 (+2)
More than you would think - a lot from kitchen, some from (newer) furniture, some faecal matter from mites, house dust which is largely human skin, cleaning chemicals, ozone, positive ions (the bad ones) from laptops especially Macbooks, mould spores, etc.
www.blf.org.uk/support-for-you/indoor-air-pollution/causes-and-effects
www.epa.gov/indoor-air-quality-iaq/introduction-indoor-air-quality
but in may countries the original source of 'household' (indoor) air pollution is actually from outside the home:
www.conserve-energy-future.com/causes-and-effects-of-indoor-air-pollution.php
www.ncbi.nlm.nih.gov/pmc/articles/PMC5089137
I bought two HEPA filters to help protect others during a home isolation, but I also had in mind that it would be useful afterwards!
Derek @ 2021-11-19T18:27 (+1)
Thanks - this is useful and I will explore some of the suggestions.
Is there much research comparing immediate vs extended release melatonin? E.g.:
- Is IR better for speeding sleep onset, as one might expect?
- Does XR actually improve sleep maintenance/duration more than IR?
- Do they have the same effect on sleep efficiency?
- Is the optimal dose the same for each?
- Dose aside, do combined IR/XR supplements, or taking a bit of each, give you the 'best of both worlds'?
RayTaylor @ 2022-01-11T00:00 (+3)
The decision may be between IR melatonin and ER 5-HTP which is a precursor:
www.foodstuffs.ca/scrapbookmain/2017/5/14/5-htp-vs-melatonin
"For some people, taking melatonin will help induce and maintain sleep. However, melatonin supplements usually only work if a person has low levels of melatonin in their system (this situation is commonly found in elderly persons). In other words, if you have normal levels of melatonin, taking melatonin supplements won't be as effective in helping you sleep.
That's where 5-HTP comes in. Since it works on serotonin as well (and indirectly on melatonin), it may be a better supplement to take for individuals with normal levels of melatonin that are suffering from insomnia. Because it interacts with serotonin, people who are already on anti-depressants or MAOIs should talk to their doctor before trying 5-HTP (melatonin, on the other hand, is generally safe to use with these other drugs when taken as directed)."
www.quora.com/What-is-the-difference-between-taking-melatonin-and-5HTP
General intro to 5-HTP and uses:
www.mountsinai.org/health-library/supplement/5-hydroxytryptophan-5-htp
Derek @ 2022-01-11T17:17 (+1)
Thanks. I tried 5-HTP a few years ago and didn't notice any benefit, but maybe I'll give it another go.
newptcai @ 2021-11-18T12:52 (+1)
Don’t forget sleep apnea. I recently got a diagnosis and treatment. Felt much better now.
Bryan Hanlon @ 2021-11-18T02:31 (+1)
Thanks for this post, and for the links to SSC and Gwern. I just ordered some 1 mg Melatonin and plan to cut it in half to start.
I’m a pretty poor sleeper, both with falling asleep and staying asleep. I suspect I’ll also benefit from establishing a similar routine for both weekdays and weekends, which tend to pretty distinct right now.
KevinO @ 2021-11-17T18:15 (+1)
I appreciate this writeup! Some of the interventions and insights were new to me even after attempting my own research in to improving sleep quality.