Snakebites kill 100,000 people every year, here's what you should know
By MathiasKB🔸 @ 2022-04-27T14:30 (+319)
WHO estimates between 81,000-138,000 die every year from venomous snakebites. What on earth!? When I first heard this I refused to believe it. How had I managed to call myself an EA for so many years and not known snakebites were this big a deal? Not only do snakebites kill an unfathomable number of people, another four hundred thousand are permanently disabled every year.
In this post I will:
- Provide an overview of the situation.
- Look at the cost-effectiveness of conventional interventions to prevent and treat envenoming.
- Argue that a new medical invention could make a massive difference and shill for the company that invented it.
Why do snakebites kill and maim so many?
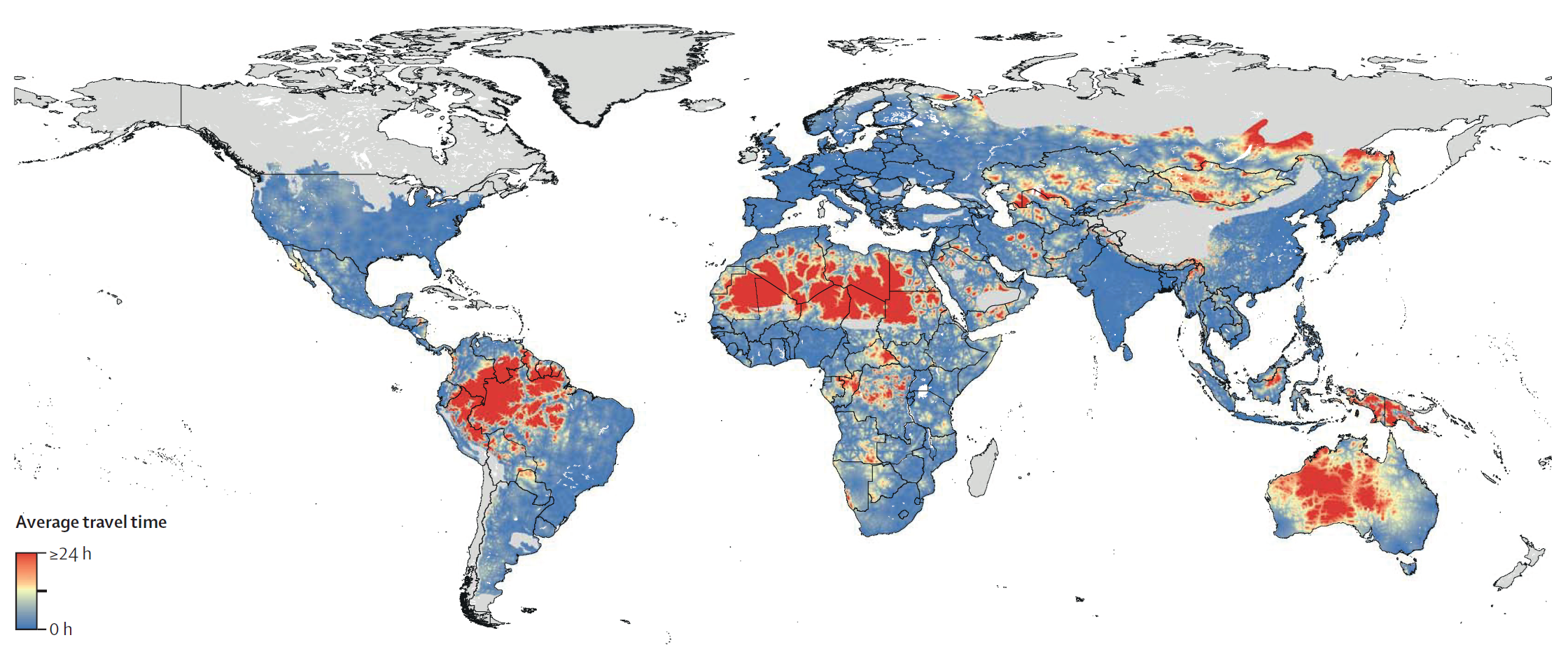
Imagine you're a farmer working in the amazon. One day, as you are working your field, you suddenly feel a searing pain from your leg. You see a snake dislodging its fangs from your calf and quickly slither away. Was it venomous or not? Even if it were a venomous snake that bit you, there's a 50% chance it was a dry-bite, and that the swelling will go away after a while. The trip to the nearest medical facility will take an entire day and cost you a fortune. You decide to wait and see. After a while the symptoms get worse and you decide to consult your family. They tell you to go to the town's spiritual healer, who can treat you for a much smaller cost. When morning comes around, you finally make the decision to go to the hospital. It's now too late. By the time you arrive the venom will have done its damage. Even if you receive the correct antivenom treatment and survive, you will suffer permanent disability and be in for a long and expensive hospital stay. After a few weeks spent recovering in the hospital you will find yourself handicapped, out of work, and in debt.
Snakebite envenoming is an enormous burden on tropical regions in the third and second world. Like other neglected tropical diseases, the burden of snakebites is much larger than the just deaths they cause. Having a productive member of one's family or community suddenly die or become permanently disabled wrecks havoc on all those who were dependent on them. Children, for example, are often removed from schools to make up for the lost income and additional person who must now be taken care of.
After reading up on various studies, WHO reports, and meeting with the CEO of a venom diagnostics startup, I believe there are two primary reasons why snakebites do so much harm.
Snakebites are expensive to treat
Treating envenoming requires administering antivenom which is expensive to produce. Each type of venomous snake species requires its own antivenom. Administering the wrong antivenom is costly and harms the patient.
The hospitalization and antivenom treatment is far too expensive for many to afford. In Bangladesh, nearly 75% of snakebite victims spent their savings on treatment and over 60% had to borrow to meet the costs.[1]
The world currently produces roughly half the antivenom needed to treat every patient. WHO argues (without using these exact terms) that there is a lemons-market for antivenom, where production of low-grade and ineffective antivenom is crowding out high-quality producers. This has reduced the profitability of antivenom production and prevents producers from scaling up production. For example, FAV Afrique, a dependable and widely distributed antivenom in sub-saharan Africa, was discontinued in 2016. I haven't been able to verify that recent discontinuations of antivenom production can be attributed to a lemon market, and an alternative explanation could be that WHO is neglecting that a worse treatment for less money may be the better outcome for some.
Lemons-market or not, we need to produce much more antivenom at a much lower cost.
Snakebites are difficult to diagnose
Diagnosing snakebites in the third world involves waiting for the patient to show symptoms and having a well-educated doctor attempt to determine the species of snakebite based on the patient's symptoms, bite-marks and geography. This process has many points of failure and misdiagnosis is common. The waiting time for the patient to develop symptoms alone delays the treatment by vital hours and lowers the chance of a complete recovery.
Due to the difficulty of diagnosing and cost of misdiagnosis, antivenom is often only available at larger clinics where doctors are trained to diagnose and administer it. For patients this means having to travel great distances to get treatment, by which the odds of survival have decreased.
I found this paper to be a great overview of the diagnostics landscape around the world.
Effectiveness of conventional interventions
Effectively treating snakebite simply requires healthcare capabilities much beyond what many third world countries can provide. Improving these healthcare capabilities often requires multiple steps to be taken at simultaneously which is exceptionally difficult to do.
Doctors of local clinics must become better able to diagnose snakebites to justify administering antivenom. Local clinics can't justify improving their diagnosing of snakebites if they don't have the antivenom to treat their patients. Solving one bottleneck often gives rise to another.
For reasons I don't quite understand, RCT's and other studies on snakebites are exceptionally difficult to conduct, meaning there is large uncertainty surrounding basically everything related to snakebites. This difficulty in conducting studies is emphasized by multiple reports and everyone I spoke with on the matter.
Despite this uncertainty, there are studies on the cost-effectiveness of available treatments that suggest conventional treatments may reach effectiveness in the same order of magnitude as givewell's recommended charities.
Cost-effectiveness of antivenom treatments
The most straight-forward treatment is simply to pay for antivenom and its distribution.
This was the best study I found on estimating the cost-effectiveness of antivenom treatments. The authors create a decision-tree of snakebite outcomes and run monte-carlo simulations to estimate the cost-effectiveness of treatments.
They found the cost to be $1997.91 per death averted in the most effective sub-saharan country, to $6204.95 in the least. That is $82.63-256.61 per DALY. For reference, Givewell's recommended deworming programmes are in the range of $30-80 per DALY.
The study has its limitations, with many uncertain estimates of important variables. But until better studies and RCT's for antivenom treatments are made, this study is likely the best estimate of cost-effectiveness available.
Snakebite awareness radio outreach
In many communities 60-80% of snakebite victims choose traditional medicine or spiritual healers instead of hospital treatment.[2] People likely do this due to a mix of cultural pressures and lack of information. Radio-based outreach campaigns for other topics can be highly effective. It may be that information related to prevention and treatment of snakebites can achieve similarly effective results.
WHO emphasizes the importance of community engagement in their 2030 to reduce deaths. I would be excited to see someone do further work in analysing why radio-based outreach is so effective for certain domains and whether we should expect snakebites to be one of those domains.
A new innovation in venom diagnostics could be a game changer
After recovering from my initial shock, I discovered that one of the world's leading labs working with envenoming is located in Denmark where I live. I met with one of its researchers, who recently founded the company Venomaid. They have developed a cheap lateral-flow test that reliably detects envenoming even before symptoms appear.
This test enables anyone to reliably diagnose the species of snakebite. Such a test would enable rural medical personnel to accurately diagnose and administer the correct antivenom.
This seemed too good to be true. If diagnostics is this big a bottleneck and the test is as cheap and reliable as venomaid claims, why hasn't WHO, for example, adopted it into their 2030 plan which heavily emphasized improving clinics diagnostics capabilities? WHO's plan was launched in 2019, and has been in the works well before that. Venomaid's lab produced the world's first working lateral-flow test to detect envenoming in 2018. WHO's strategy doesn't include anything like this as a crucial component, because they didn't know it could be done.
There's many reasons to have reservations over whether it will be cost-effective. Even if the test is inexpensive, what is the cost of distribution? How much training do clinics need to administer the test? To what extent will the test alleviate the diagnostic bottleneck that is supposedly preventing roll-out of antivenom to local clinics?
I initially held many of these reservations (and still have many!), but felt I was receiving satisfying answers to most of them. For example, the entire world has just received a crash-course in producing, distributing, and using lateral-flow tests due to covid, significantly lowering many costs associated with Venomaid's test.
Venomaid's own cost-effectiveness estimate (which they claim is conservatively calculated, but seems optimistic to me) is ~20 USD/DALY for Brazil, the first country in which they plan to roll out their product.
Despite the uncertainties I believe their lateral-flow test looks both incredibly promising and neglected in its current stage. I am willing to bet money at good odds that lateral-flow tests to diagnose snakebites will be commonplace within a few decades.
They are hoping to raise $2M for their next seed round following their pilot project in Brazil, but it seems to me that if concerns over profitability and funding were less of a concern they would be able to scale much faster. If a philanthropist were to offer a large buy-order conditional on a study estimating its cost-effectiveness or something similar, they would be able to scale up and start saving lives much faster.
I hope this post will inspire some organisation to look further into this and figure out if it really is as promising as it looks to me.
- ^
- ^
page 19 of the WHO 2030 Report
Wind @ 2022-04-27T14:47 (+58)
For reference malaria killed 600.000 in 2020 according to WHO, so it is pretty surprising to me that I've never heard of snakebites given that they kill about 1/6th of what malaria does (not to mention the handicapping).
Super interesting writeup, I'm glad that my horizon is now a little wider.
Pat Myron @ 2023-05-15T18:39 (+1)
Wider list if anyone's curious what's after mosquitos and snakes:
https://en.wikipedia.org/wiki/List_of_deadliest_animals_to_humans
jablevine @ 2023-08-07T13:03 (+43)
Summary: Good news!! If you read this post last year, about 50,000 fewer people are dying each year than you thought.
I'm very sceptical of the WHO estimate of 81,000-138,000 annual fatalities. Following the citations:
- That WHO stat (citation 6 in the report linked in footnote 2, note that link automatically downloads a pdf) cites Gutierrez et al. 2017.
- Gutierrez et al. have a range of 81,410 to 137,880. This range is not a confidence interval, but "combined upper estimates of mortality" (page 2) — meaning these numbers are each upper bounds. Gutierrez et al. have two citations for the range, Kasturiratne et al. 2008 and Chippaux 1998.
- Kasturiratne et al.'s "high estimate" is 93,945 deaths per year. They come to this number by averaging rural and urban incident/fatality rates in a way which I don't agree with,[1] and applying regional fatality rates to areas without data.[2]
- In Chippaux, the largest number I can find is 125,345. Despite the specificity, this paper relies heavily on round numbers.[3] Also, the paper is 26 years old, and the number of people employed in agriculture (top risk for snakebites) has fallen by more than a third.
- I have no idea where the 137,880 number in Gutierrez et al. comes from, and therefore where the WHO got that figure, and therefore where the number in this post comes from. It's widely cited to the WHO report, but I lose track of it before Gutierrez et al.
What numbers seem more reasonable? From the 16-year-old Kasturiratne et al. paper, I find their low estimate (19,886 annual deaths) too low, so I'd accept their range of 19,886 to 93,945 as a acceptable confidence interval (90% for the year 2007). The Chippaux numbers are much too high, and the higher Gutierrez et al. number is entirely unsourced. Further, as noted above, the decline in agricultural labor over the past two decades will have reduced exposure to snakes, and the rapid expansion of medical care in rural India will have further addressed the problem.
Thankfully, the 2019 GBD report[^5] did a much better job (imo) of estimating this. Their value estimate for all deaths from venomous animals is 79,700, and venomous snakes is 63,400.[4] This seems much more reasonable, though GBD figures do have a history of being too high, and I personally revise my median estimate down to 55,000.
[1] They assume that all rural areas have the highest incident and fatality rate, which seems obviously untrue. But to create an upper bound when dealing with lots of missing data, fine.
[2] "Our approach minimised this effect [of ignoring regions with missing data], although in some regions, such as the Caribbean, lack of data still meant that we were forced to use very high rates in our calculations of the high estimate." (page 1601)
[3] 80% of this high estimate relies on this paragraph:
"In Asia (population, ca. 3500 million) as a whole there may be up to 4 million snake-bites each year, of which almost 50% are envenomed. Approximately half of the victims reach hospital and the annual number of deaths resulting can be estimated at 100000."
The 100,000 number is not justified any further.
[5] I used the query tool here; you need to make a free account.
[4] This leads to the question, what other other venomous animals are killing 16,000 people per year? I couldn't find an easy answer; my guesses in order are scorpions, jellyfish, and spiders. I highly recommend Venomous by Christie Wilcox for a cultural and scientific history of venom.
MathiasKB @ 2023-08-08T08:29 (+6)
These are the comments I come to the EA Forum for!
It wouldn't be the first time I've seen the WHO reports on snakebites get something blatantly wrong. If I recall correctly, they accidentally flipped a figure for percentage of people who couldn't afford treatment in the Bangladesh study.
Did you look into the Indian one million death's study? As far as I remember, that was the study which led WHO to revise their previous global estimate of 50k, as it found 50k annual deaths to snakebites in India alone.
If you have, I'd be curious to get your take on how much weight to put on it. My understanding is that if not for this study, WHO's estimate would be around what you arrived at.
NickLaing @ 2023-08-07T13:38 (+1)
Great wee analysis here - in future this kind of thing might be better posted on your "quicktakes", or maybe there as well because otherwise it could well get lost quickly on the forum and few might see it.
Peter Wildeford @ 2022-04-28T21:02 (+19)
Does anyone know if there are any ways to direct funding to this? I'd be potentially interested in exploring it.
MathiasKB @ 2022-04-29T07:33 (+6)
When I first learned about the diagnostics startup, my immediate thought was that some EA Fund would be interested in further evaluating it. Unfortunately neither Open Philanthropy, EA Funds, or FTX Community are currently accepting unsolicited proposals.
The primary reason I wrote this post was to get the attention of fund-managers, and hopefully get someone to figure out if this is impactful and fund it if it is.
Jorgen_Ljones @ 2022-04-29T09:17 (+4)
Aren't OpenPhil? https://www.openphilanthropy.org/giving/how-to-apply-for-funding#Can_I_apply_for_a_grant
They specify that they have low expectations for unsolicited proposals, but it's possible to contact them about it.
MathiasKB @ 2022-04-29T13:54 (+5)
The page linked in my comment states that they are not currently accepting unsolicited proposals, but I agree the FAQ makes it sound like they are open to being contacted. My guess is there probably isn't a clear cut policy and that they just want to avoid setting an expectation that they will evaluate everything sent their way.
Will send them a message, thank you :)
Peter Wildeford @ 2022-05-03T15:21 (+2)
EA Funds definitely accepts unsolicited proposals! That's the whole point of it!
Lorenzo @ 2022-05-03T15:40 (+6)
You would think so, but the Global Health and Development Fund is basically GiveWell seed grants
https://funds.effectivealtruism.org/funds/global-development#faq
Can I apply for funding to the Global Health and Development Fund?
The Global Health and Development Fund is not currently accepting applications for funding.
I don't think there's any Global Health fund that accepts proposals, maybe the closest thing is this Nonlinear ideas spreadsheet? https://docs.google.com/spreadsheets/d/1uNcKi5xjJinBzeiBv0SKVekoTCM6TLkd-GKA7HSjMEU/edit#gid=478371070
Peter Wildeford @ 2022-05-03T16:14 (+11)
I'd be willing to fund these sorts of things via the Effective Altruism Infrastructure Fund
Lorenzo @ 2022-05-04T09:55 (+2)
Thanks!
I'm trying to understand the structure of the EA funds, isn't "direct work" outside of the scope of the Infrastructure Fund?
> this Fund supports work that could multiply the impact of direct work, including projects that provide intellectual infrastructure for the effective altruism community, run events, disseminate information, or fundraise for effective charities
Have you funded "direct" global health interventions in the past?
Peter Wildeford @ 2022-05-04T15:10 (+12)
I agree it is confusing but I prefer to just fund impactful things and worry less about what fits in the scope of the fund. And even if the other fund managers deem it out of scope, I frequently can refer it to other interested funders.
Lorenzo @ 2022-05-04T15:27 (+1)
Interesting, thanks!
Do you happen to have in mind a recent example of a non-infrastructure intervention that was funded directly or indirectly through the Infrastructure Fund?
Peter Wildeford @ 2022-05-04T16:31 (+3)
The best example I have right now is that I funded a climate change research group but arguably research is still infrastructure... I'd like to fund some more direct stuff though
MathiasKB @ 2022-05-03T16:13 (+2)
They are currently explicitly writing on the page I linked that they are not.
Can I apply for funding to the Global Health and Development Fund?
The Global Health and Development Fund is not currently accepting applications for funding.
If that is not the case, I'm not too happy with their communication!
EDIT: whoops, didn't see Lorenzo's comment
John Bridge @ 2022-06-12T17:07 (+18)
I'm a bit late to the party on this one, but I'd be interested to find out how differential treatment of indigenous groups in countries where snakebites are most prevalent impacts the tractability of any interventions. I don't have any strong opinions about how significant this issue is, but I would tentatively suggest that a basket of 'ethnic inequality issues' should be considered a third 'prong' in the analysis of why snakebites kill and maim so many people, and could substantially impact our cost-effectiveness estimates.
Explanation:
The WHO report linked by OP notes that, in many communities, over 3/4 of snakebite victims choose traditional medicine or spiritual healers instead of hospital treatment. I don't think this is a result of either of the two big issues that the OP identifies - it doesn't seem to stem from difficulty with diagnosis or cost of treatment, so much as being a thorny problem resulting from structural ethnic inequalities in developing countries.
I'm most familiar with the healthcare context of Amazonian nations, where deeply embedded beliefs around traditional medicine and general suspicion of mestizo-run governments can make it more difficult to administer healthcare to indigenous rainforest communities, low indigenous voter turnout reduces the incentives of elected officials to do anything about poor health outcomes, and discriminatory attitudes towards indigenous people can make health crises appear less salient to decisionmakers. Given that indigenous groups in developing countries almost universally receive worse healthcare treatment, and given that much indigenous land is in regions with high vulnerability to snake envenoming,[1] I wouldn't be surprised if this issue generalised outside of Amazonia.
{kind=link}
Depending on the size of the effect here, this could considerably impact assessments of tractability. For example, if developing country governments won't pay for the interventions, it might be difficult to fund long-term antivenom distribution networks. Alternatively, if indigenous groups don't trust radio communications, communicating health interventions could be particularly difficult. Also, given the fact that 'indigenous' is a poorly-defined term which refers to a host of totally unrelated peoples, it might be difficult to generalise or scale community interventions.
MathiasKB @ 2022-06-12T18:21 (+2)
Thanks for the comment, I'd like to know that as well!
Since writing the article and diving further into the antivenom crisis, I think I've actually doubled down on cost of treatment being the primary issue.
When faced with the following options:
1. long trip to clinic, expensive treatment that may not work.
2. short trip to local healer, inexpensive treatment that may not work
I can understand why someone would opt for the latter.
My model would be that people would become much more willing to go to the hospital for , when they see acqaintance after acqaintance come back healthy, happy, and with their wallets intact as opposed to in coffins with a bill attached.
One way to test this, could be to look how people's willingness to go to the hospital changes when cheap and working antivenom is introduced in an area. Another way could be to look at how prevalence of inefficacious (or outright fraudulent) antivenom affects willingness to go to the hospital, though I suspect there isn't sufficient data to do this analysis.
That said I feel very uncertain about my prediction, and I don't think I'd be willing to make a bet with particularly good odds. Frankly I don't know anything about indiginous communities or their circumstances, and I'd trust your judgement more than mine. The fact that WHO's 2030 plan spends such a large proportion of its resources on community engagement suggests it's a bigger deal than I made it to be.
rileyharris @ 2022-04-28T00:55 (+13)
Thanks for the post - this seems like a really important contribution!
[Caveat: I am not at all an expert on this and just spent some time googling]. Snake antivenom actually requires that you milk venom from a snake to produce, and I wonder how much this is contributing to the high cost ($55–$640) of snake venom [1]. I wonder if R&D would be a better investment, especially given the potentially high storage and transport costs for snake venom (see below). It would be interesting to see someone investigate this more thoroughly.
Storage costs are pretty low in that cost effectiveness estimate you cite [2], but it seems pretty plausible to me that storage and transportation costs would be much higher if you wanted to administer snake venom at smaller clinics that were closer to the victims of snake bites. The cost was based on this previous estimate, in which they say“The cost of shipping from abroad where the antivenoms are manufactured, transportation within Nigeria and freezing of antivenom (including use of supplementary diesel power electric generators in addition to national power grid) is estimated at N3,000 ($18.75) from prior experience and expert opinion. But it was assumed that appropriate storage facilities already exist at the local level through immunization/drug services and that no additional capital investment would be required to adequately store the antivenom in the field” [3].
I'm not sure exactly what facilities are required and how expensive they would be, but this seems like it could be an important consideration.
[1] Brown NI (2012) Consequences of neglect: analysis of the sub-Saharan African snake antivenom market and the global context. PLoS Negl Trop Dis. 6: e1670.
[2] Hamza M, Idris MA, Maiyaki MB, Lamorde M, Chippaux JP, et al. (2016) Cost-Effectiveness of Antivenoms for Snakebite Envenoming in 16 Countries in West Africa. PLOS Neglected Tropical Diseases 10(3): e0004568. https://doi.org/10.1371/journal.pntd.0004568
[3] Habib AG, Lamorde M, Dalhat MM, Habib ZG, Kuznik A (2015) Cost-effectiveness of Antivenoms for Snakebite Envenoming in Nigeria. PLOS Neglected Tropical Diseases 9(1): e3381. https://doi.org/10.1371/journal.pntd.0003381
Jesper Magnusson @ 2022-05-19T22:57 (+5)
I was also thinking of the high production costs as a potential area of intervention. A few minutes of browsing turned up some potential advancements in production methods of antivenom, e.g. using synthetic biology, and I would be interested in learning about the potential cost-effectiveness of implementing or scaling up such alternative production methods. It seems like many of them are still in the R&D-stage though, but this could be an area to keep a close eye on.
A recent article on the topic:
https://www.drugdiscoverynews.com/snakebite-antivenoms-step-into-the-future-15378
MathiasKB @ 2022-05-20T06:22 (+3)
Since writing this article, this is actually one of the things I've been looking into! I think it looks very promising, as many of the issues outlined by WHO seem downstream from people simply being unable to afford high quality antivenom. (ie. why do people choose local healers? Because hospitals cost more and don't help either!)
It also looks like the marginal cost of high quality antivenom would decrease up to an order of magnitude if you scale up production. I have yet to take an in depth look at synthetic antivenom production, but after briefly looking into it, it seems that we are not going to get synthetic antivenom just yet.
John Litborn @ 2022-04-28T09:58 (+2)
If the lateral-flow test can be cheaply produced, distributed and stored at smaller clinics - then you might be able to then quickly drive patients to larger clinics once positively diagnosed and might not then have to worry as much about the larger costs of the anti-venom. Will depend a lot on the time/distance to nearest larger clinics though.
Annette Nakakande @ 2023-02-13T18:10 (+10)
Quite educative! Thank you for this information. Are there any preventive measures used?
In Uganda (which is in the tropics), there is potential to see many snakes. in order to prevent such occurrences, there is sensitization about removing bushes and trimming all grassy areas regularly.
Furthermore, there are some plants which are used to prevent snakes from getting into homesteads, farms, etc. These include what are called "snake plants", tobacco plants, etc., which are planted around farms and homes. That is the local way of keeping snakes away.
JoelMcGuire @ 2022-04-28T00:16 (+8)
Very nice post. Snappily written and information-dense. With a quick scroll, I feel like I learned a lot. I would really like more posts like this. Thank you!
AndreaM @ 2022-04-27T15:07 (+8)
Thanks for this writeup! I definitely never thought about snakebites as a major issue before, despite its similarity to "obvious" global health issues like malaria.
Finngoeslong @ 2022-05-14T14:59 (+7)
Really interesting summary, thanks for sharing. Whilst not an expert, I've done some work in past with diagnostics in developing countries in Africa.
It's common for manufacturers to make big claims about their technology, but what's crucial is having independent evaluation/certification from regulators.
In the case of snake bites, I would imagine its tricky to prove the test works. Not easy to find snakebite victims in time.
I had a look at the venomaid website and didn't see anything about whether they had approval for their tests. That can take a long time.
Happy to collaborate on this and ask around the diagnostics people I know if interested?
ColdButtonIssues @ 2022-04-27T21:38 (+6)
Fascinating. Have any public health departments tried snake extirpation in certain areas? (Or is that an obviously flawed approach?)
Cienna @ 2022-04-28T14:51 (+9)
If you had other small predators around to keep the rodent populations in check, such as weasels and hawks, maybe you could get away with removing snakes. Rodent population booms are undesirable because rodents carry diseases which can be infect humans, pets, and livestock. Rodent poison isn't a good alternative because the poisons also kill scavengers (dogs, owls, etc.) that eat the poisoned rodents, and are harmful at sub-lethal doses. Birds of prey aren't enough to keep a rodent population in check because they can't access most of the places where rodents like to hide, so predators are also needed which can travel along the ground and enter burrows.
Predator removal has been tried repeatedly, usually with negative consequences on the ecosystem. Australia in particular has lots of case studies about humans trying to manage small pests without enough predators, and Yellowstone has a famous case study about the value of reintroducing predators. Keeping predators around is unpleasant, but the human effort involved in compensating for their absence is expensive.
I think keeping the non-venomous snakes mostly covers this concern though!
The only upside I know of provided by venomous snakes specifically is that they are a source of very complex specialized proteins with potential medical applications, such as anticoagulants and vasoconstrictors.
Ramiro @ 2022-04-27T23:08 (+4)
I don't think environmentalists would like it
Cienna @ 2022-04-28T14:56 (+5)
Oooh, I'm hopeful this technology could be used for identifying insect stings too! Insect antivenom faces some similar challenges.
Peter S. Park @ 2022-04-28T20:29 (+4)
What about something they can wear on their leg to prevent the snakebite?
MathiasKB @ 2022-04-29T07:20 (+3)
I wondered about this as well. There's no doubt that it would reduce snakebites, but whether it's cost-effective is more difficult to tell.
An analyst I spoke to pointed out to me that after all it's still pretty rare to be bitten by a snake. The amount of footwear you'd need to distribute per snakebite prevented is pretty high, and likely pretty expensive.
Peter S. Park @ 2022-04-29T16:25 (+1)
That makes sense! Shoes are probably more expensive than malaria nets.
But it might still be a better intervention point than antivenom+improving diagnosis+increasing people's willingness to go to the hospital.
AndrewDoris @ 2022-05-15T02:50 (+5)
I suspect it would be easier to convince people who HAVE been bitten by a snake to go to the hospital than it will be to convince people who have not yet been bitten by a snake to constantly wear some kind of protective wraparound shinguards every time they're on the farm. The daily inconvenience level seems high for such a rare event. Even malaria nets are often not used for their intended purpose once distributed, and they seem to me like less of an inconvenience.
Pat Myron @ 2023-03-14T06:49 (+1)
@Peter S. Park @MathiasKB @AndrewDoris
rather than armoring where you're bit, less costly / inconvenient preventing bites in the first place by emitting odor / noise / light to ward off predators. Odor seems most promising for snakes according to https://www.callnorthwest.com/2019/04/home-remedies-to-keep-snakes-away/
Maybe more than superstition to carry around smelly garlic / onions :)
aaronmayer @ 2022-04-28T00:14 (+4)
Thank you for sharing this! It's always so heartbreaking to learn of something new that causes so much pain and suffering, but identifying it is the first step to ameliorating it! Hoping some plucky and dedicated EAs take this on as a potential cause area, and the radio + testing combination seems like a great place to start!
MarisaJurczyk @ 2022-04-28T18:42 (+3)
99% Invisible had a podcast on this that I found really interesting. The scale of the problem must have gone completely over my head. Great write-up!
Isaac King @ 2022-04-28T00:34 (+3)
multiple steps to be taken at simultaneously
Typo
Rockwell Schwartz @ 2022-04-29T18:19 (+2)
Thank you for this write-up! I want to flag that in addressing this problem and possible solutions, there are also significant implications for (wild) animal suffering—e.g. Rileyharris's note about antivenom requiring "milking" of captive snakes and Cienna's comment about predator-play interactions—and I would hope any solution would take this into account in a meaningful way.